Building MR-simulation competency in radiotherapy
FieldStrength MRI magazine
User experiences - November 2019
Starting from scratch, The Christie develops a MR-sim education and training program for proton beam radiotherapy service
In the development of the National Health Services’ first high energy proton beam therapy (PBT) center at Manchester’s The Christie Hospital, acquisition of a dedicated MRI system for PBT planning was essential. MRI can provide exceptional soft tissue visualization for precise target and organs-at-risk (OAR) delineation for treatment planning and monitoring on-treatment variation – an imperative for safely delivering proton therapy.
However, integrating MRI in a radiotherapy department presented a challenge – radiotherapy personnel typically have little or no experience in safely and effectively operating in an MRI environment, while diagnostic radiographers have no or limited exposure to the needs of pre-treatment radiotherapy. To enable the safe, smooth implementation of an MR-sim Service, the Christie team developed and executed a training and education program for all PBT employees.
“The biggest problem in ensuring the safe and smooth implementation of an MR-sim service was a lack of knowledge, experience and training”

The Christie NHS Foundation Trust
The Christie NHS Foundation Trust in Manchester, UK is the largest single site cancer centre in Europe, treating more than 44,000 patients a year. The centre has access to 15 linear accelerators and offers both proton beam therapy and MRI guided therapy.
The Christie pre-treatment staff of the Proton Beam Therapy Center consists of:

Thomas Edwards is pre-treatment principal radiographer for protons at the Christie NHS Foundation Trust and has worked in radiotherapy for 16 years, specializing in radiotherapy imaging. Edwards, who was involved in the development of the Christie Proton service, was among the first radiographers recruited and supported various aspects of the implementation. These include procurement of the service’s Ingenia MRRT 1.5T system, service development, recruitment, training and service provision. He also played a lead role in implementing a series of firsts within radiotherapy, including extensive work in development of MRI in radiotherapy implementation at NHS Trust.
Starting at ground zero
While The Christie’s Ingenia MR-RT 1.5T system was to be the centerpiece of the new PBT facility’s pre-treatment workflow, establishing an imaging staffing model for the department and training those who would operate the MRI were major hurdles that department administration would need to overcome. “The biggest problem was a lack of knowledge, experience and training,” says Thomas Edwards, Principal Radiographer at The Christie, who lead the team in developing education and training. “Therapeutic and Diagnostic Radiographers in the UK are on completely different educational paths so each group knew little about the other’s profession, yet the expertise of both roles was required for safe, competent pre-treatment imaging. Cross-training was clearly needed.”
This challenge is further complicated by the fact that although in the UK there are non-compulsory post-graduate MRI qualifications,
the approach to educating even diagnostic radiographers in MRI falls heavily on individual departments to set standards in MRI training and education. This makes it difficult to know where to start in a radiotherapy department. “The Society of Radiographers [SCoR] indicates, for example, that an individual who can scan with MRI is ‘An authorized person deemed to have sufficient experience (knowledge and skills) and appropriate training and is responsible for operating the scanner in a safe and appropriate manner,’” he says. “The challenge was, that there was no guidance as to what defines that ‘knowledge” during the development of our service. However, this is changing, and a working party has been developed by the Society to publish guidance and an overview of the educational and professional requirements for safe, effective use of MRI in radiotherapy for the purposes of simulation and on-board radiotherapy guidance.”
Therapeutic and Diagnostic Radiographers in the UK are on completely different educational paths so each group knew little about the other’s profession”
First steps in building MR-sim competence
A full year before the complete pre-treatment staff were hired and ready for training, Edwards became involved in acquiring the MRI system in a competitive tender process. To facilitate this process, Edwards recruited Lisa McDaid, a diagnostic radiographer with abundant MRI experience to join the standard procurement team, which included a physics lead, radiotherapy engineer, MR physicist, radiologist and a project manager. “Since I had very little MRI experience, we needed to hire someone to help us procure the system,” he says. “Lisa’s MR oncology experience and her familiarity with a variety of MRI systems was invaluable in evaluating modern MRI scanners.” McDaid also played several other key roles after the Ingenia acquisition and prior to recruitment of the PBT diagnostic superintendent radiographer and MR responsible person. These included ensuring that The Christie was aligned
with “MR local rules” governing regulatory requirements for safety in the PBT department; helping recruit the therapeutic and diagnostic radiographers comprising the permanent PBT pre-treatment team; assisting in identifying training needs; safety training; and developing the initial sequences with the Philips applications training team and other pre-treatment team radiographers.
With the delivery of the Ingenia MR-RT in December 2017, the clock started for the clinical go-live of the PBT center. “The machine had to be installed, tested and commissioned and we still had to recruit many of the pre-treatment staff members before we could start applications training,” Edwards says. “The schedule was very tight. Our first patient was planned for December 2018, which left only nine months to complete training.”
Timeline Building MR - sim service - The Christie
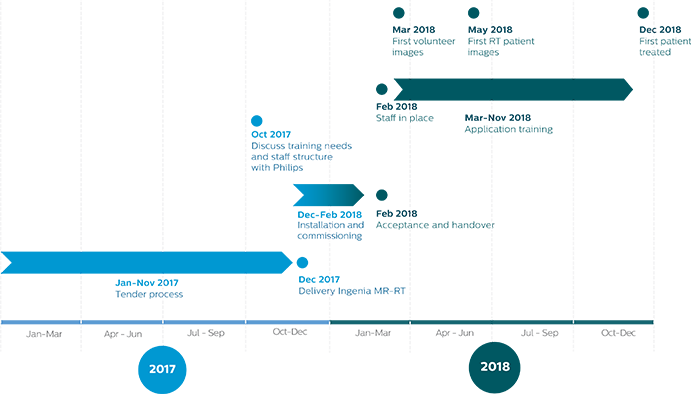
Figure 1. Timeline of building MR-sim service at The Christie Proton Beam Therapy Centre.
Determining a staffing model
“We decided that we should always have a 50-50 split of diagnostic and therapeutic staff,” Edwards says. “And, as we came to post and started looking at staffing and anticipated workload, The Christie team agreed that we needed to have a mix of both professions, and that ideally each group needed to be cross-trained in MRI and radiotherapy to create hybrid MR-RT radiographers. We always assumed that MR-RT scanning would require a collaborative practice, so at minimum there would be one diagnostic radiographer and one therapeutic radiographer at any time to scan the patients.”
The Christie proton project team and NHS had worked together to define the PBT center’s staffing model, including the make-up of the pre-treatment staff who would operate the MRI system.
MR-RT applications training: the first form of competence
By February 2018, the Ingenia system was commissioned, fully accepted and handed over, and the staff had been recruited and hired – a complement of three therapeutic and three diagnostic radiographers. Philips application training began in March, first for the physicists, engineers and dosimetrists, then for the permanent pre-treatment staff.
Two months before the delivery of the Ingenia MR-RT, The Christie team met with Philips representatives to confer on staff structure and training needs for the diagnostic and therapeutic radiographers.
"The didactic and hands-on Philips applications training was really well structured"
“The didactic and hands-on Philips applications training was really well structured, with a modular setup in chapters, key stages and key points of the process,” Edwards observes. “It was quite comprehensive as well, including everything from safety and basic operations to developing and modifying protocols. Over a six-week period, they led us through what we needed to know about Ingenia MR-RT. And, although the training was very well aimed at the therapeutic radiographers, the diagnostic radiographers also benefited because they had limited understanding of this particular system. “Since the applications training was the first form of competence, it was extremely important that it was well-documented and assessed, to enable us to show evidence of the training – especially in lieu of other formal accredited training,” he adds. “The training was excellent. The Philips’ applications specialist, Lynsey Cameron-Clark, and The Christie team developed a fantastic relationship, which was reassuring. And we felt comfortable calling on her repeatedly – in fact, we still do.”
Hub-and-spoke model provides tailored training for different groups
Following applications training, The Christie MR radiographer and Education Team worked together in order to develop the in-house training of the pre-treatment staff. They started by investigating how the Diagnostic Imaging service trains its radiographers and documents this program, and then developed the hub-and-spoke training model for MR simulation.
“We knew what we knew, but we didn’t know what we didn’t know,” Edward says. “So we also wanted to find out where our gaps in knowledge were by relying on the Philips’ application specialist and our team of therapeutic and diagnostic radiographers. We also relied on them to identify their gaps in knowledge. For example, for diagnostic radiographers, radiotherapy patient positioning is not part of their usual scope of practice, while the therapeutic radiographers – though they were aware of radiation hazards – had little previous knowledge about the risks of projectiles in a magnetic field or the danger of scanning a patient that has an implanted medical device. Upskilling both groups presented a major challenge.”
Overview of the main learning objectives identified per job role
• Reproducibility and registration requirements • Purpose of images for treatment planning (target v. OAR delineation v. synthetic CT generation) • Differences in requirements of diagnostic and treatment planning imaging (acquired orthogonal to system, geometric fidelity, MP imaging on the same isocenter for better registration accuracy) • MRI Safety • Basic MR physics • Image acquisition (including parameters and tradeoffs, artifact recognition and reduction) • Image interpretation (e.g., understanding which sequences are used for target v. OAR delineation, anatomy) • Image interpretation • Image registration (cross-sectional/cross-modality anatomy)
For Diagnostic Radiographers
• Treatment position and coverage for treatment planning purposes (PBT requires greater accuracy)
For Therapeutic Radiographers
For Treatment Planners/Radiation (Clinical) Oncologists / Dosimetrists
We knew what we knew, but we didn’t know what we didn’t know, so our goal was to find out where our gaps in knowledge were”
The hub-and-spoke model (see figure 2) consists of a core module (hub), which comprises of the important parts of the UK’s Medicines and Healthcare Products Regulatory Agency (MHRA) MR safety guidelines.
The spokes represent additional learning modules for specific job roles, and include modules on safety, screening, scanning, daily QA and image contrast.
“We can choose which training modules are required for any role in the PBT department, and these are mapped out in the training needs analysis performed by the education team,” Edwards says. “The training priorities were safety and instilling confidence, with the ultimate goal to have the diagnostic and therapeutic radiographers be equally proficient regardless of their professional designation. In short, we wanted to create hybrid MR-RT radiographers.”
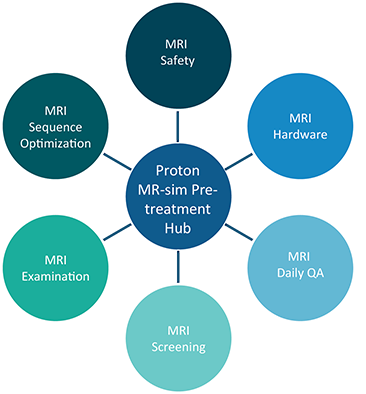
Figure 2. Overview of The Christie hub-and-spoke training model on proton MR-sim pre-treatment.
Hub pre-treatment staff and is based on MHRA guidelines: • Safety • Environment • Local rules • Equipment Each spoke includes the necessary content and consists of: • A competency profile • A guide for trainers • A guide for assessors
Proton Pre-treatment Hub includes training for MR-sim
Spoke
Contents of proton MR-sim pre-treatment spokes
| Spoke | Learning objective | Content | Who ? |
| MRI Safety | General understanding of MRI access. | • Safety presentation • Overview of MR environment | All staff working in the proton pre-treatment service |
| MRI Safety | Understanding environmental and physiological hazards of the MRI environment and how to minimise risk to patients, staff and visitors. | • Appropriate coil placement • Signal interference and/or RF burns • Use of MRI-compatible equipment • Use of hearing protection • Appropriate use of the quench button. | Radiographers working in pre-treatment Radiographers |
| MRI Hardware | Becoming competent in recognising and operating the components of the MRI system | • Use of MR coils • MR console user interface • Patient positioning | Radiographers |
| MRI Daily QA | Becoming competent in executing radiographer lead QA procedures | • Checking the laser systems • Running the periodic image quality test (PIQT) • Safety checks | Radiographers |
| MRI Screening | Ability to assess patients, staff and visitors for appropriateness of access to the MRI Suite and/or imaging | All learners must undertake a series of observed screenings to ensure patients are safe for MR imaging and be able to accurately identify the process for answering of queries regarding implants and patient conditions. | Radiographers working at the MHRA authorised user level of supervisor |
| MRI Scanning | Ability to undertake an MRI simulation examination from start to finish | Includes the knowledge, skills and competence obtained in the previous spokes and evaluates the radiographers ability to safely and efficiency put into practice all required to undertake a usable MR simulation using the most appropriate exam card and patient positioning aids for that particular treatment site. | Radiographers |
| MRI Sequence | Competence in understanding basic image formation, MRI parameters and trade-offs to be able to optimize ExamCards | Topics include: • Impact of image resolution, scan time and signal to noise ratio on each other • Acceleration factors • Difference between image type (e.g., spin vs gradient echo, 2D vs 3D, etc.) • How to recognise/minimise imaging artefacts | Radiographers |
This model ensures that all learners receive the same information, and that it’s delivered and assessed in a consistent manner”
Detailed training guides ensure consistency
“This model ensures that all learners receive the same information, and that it’s delivered and assessed in a consistent manner,” Edwards says. “The training guide contains the information to be taught, the trainer’s guide instructs how to teach the material and the assessor’s s show how to evaluate each learner’s competence. They simply ask an individual being trained to demonstrate the knowledge and hands-on skills that the trainers had presented them. We said: ‘You need to know XYZ and if you say you do, then provide evidence that you know XYZ either verbally, in writing or by a hands-on demonstration.”
The identified training needs for each group were compiled in training guides, a guide for the trainer, and an assessor’s guide. An example of a trainer's guide is shown in figure 3.
")
Figure 3. Excerpt of the Christie MR hardware training guide.
Safety in an MRI environment
Integrating MR-sim into a new department was a big change for the whole PBT service, necessitating education of more than just the pre-treatment staff. The most important aspect of this training was safety, Edwards adds. “The scanner is surrounded by 150 team members who haven’t necessarily worked adjacent to an MR scanner before,” he says. “We developed a general MRI safety program, as part of the training hub, to teach everyone working in the building about the risks associated with a strong magnetic field. Awareness of the consequences of going through a particular door or taking certain equipment into the magnet room was felt to be very important to ensure staff, patient and visitor safety.”
(See sidebar MRI Safety)
Developing Radiotherapy-specific Exam Cards for PBT Patients
The Christie team and the Philips application specialist worked with the center’s radiologists and radiation oncologists to develop PBT-specific radiotherapy planning imaging protocols (ExamCards). The process started with soliciting suggestions from the radiation oncologists regarding their image quality and contrast requirements for PBT planning.
“We used that input to develop the sequences or ExamCards and then test them on a volunteer,” Edwards says. “The primary radiologist would critique the images and the team would modify the sequences for more signal, more contrast or a different voxel size if extra detail was needed. Then we would take new images back to the radiologist for another review. It was an iterative process, but ultimately we were happy with the results.”
Once the radiation oncologists were satisfied, the center’s physicists were consulted on the images’ suitability for proton planning – their geometric accuracy and whether they could be fused with CT.
Key aspects of MHRA guidelines
MR safety
"It's not just about screening for ferrous materials or implants"
Noise • Know acceptable levels and how to limit
Specific Absorption Rates (SARs) • Know the effects of high SAR sequences • Know recommended limitations
Patient positioning and immobilization devices • Just because it’s not metal doesn’t mean it’s MRI-safe • Hidden screws and hinges • Heating effects
Anti-peristaltic and contrast agents • Training and awareness
The Christie launches proton therapy service
A journey that began in 2016 with the procurement of Ingenia MR-RT 1.5T – and continued with the recruitment of the PBT pre-treatment staff and development of a training program to transform them into MR-RT radiographers – culminated on December 31, 2018. On that date, a 15-year-old boy with a brain tumor became the PBT service’s first patient, the first of some 750 patients The Christie anticipates treating each year.
According to Edwards, the experience of creating a fully staffed PBT service from the ground up was a daunting task, but the result has been quite successful.

“There is still learning to be done, but the pretreatment team’s confidence is growing day by day,” he says. “They are a very competent team of radiographers working in MR-RT and they work fairly independently now – they ask fewer questions and are able to make decisions by themselves. The next phase will be to assess the staff again and make sure they know what we have asked them to know. It’s a whole process that needs to grow and develop, but we are confident they’re a good team of people and they are where they need to be.”
On the horizon at The Christie is a pilot program set to begin in late 2019 that consolidates educational programs for MR-sim in proton therapy, MR-sim in radiotherapy MR-linac operation in a single MR in RT hub.
“The program is designed to make sure all Christie radiographers working in MR-sim and MR-linac have enhanced skills,” he says.
They are a very competent team of radiographers working in MR-RT and they work fairly independently now”
References
2. Eccles CL, McNair. HA, Armstrong SEA, Helyer SJ, Scurr ED. (2017). In response to Westbrook - Opening the debate on MRI practioner education. Radiograph 23: S75-S76. 3. Eccles CL, NIll S, Herbert T, Scurr E, McNair HA (2019). Blurring the lines for better visualisation. Radiography 25: 91-93 4. Paulson, E., Erickson, B., Schultz, C., Li, A., (2016), Comprehensive MRI simulation methodology using a dedicated MRI scanner in radiation oncology for external beam radiation treatment planning. Magnetic Resonance Physics, Vol 42, pp. 28-39. 5. Speight R, Schmidt MA, Liney GP, Johnstone R, Eccles CL, Dubec M, et al. (2019). IPEM Topical Report: A 2018 IPEM survey of MRI use for external beam radiotherapy treatment planning in the UK. Physics in Medicine and Biology. 6. Rai R, Kumar S, Batumalai V, Elwadia D, Ohanessian L, Juresic E, Cassapi L, Vinod S, Holloway L, Keall P and Liney, G. (2017). The integration of MRI in radiation therapy: collaboration of radiographers and radiation therapists. Journal of Medical Radiation Sciences, 64(1), pp.61-68. 7. The Society and College of Radiographers & and the British Association of Magnetic Resonance Radiographers (2013). Safety in Magnetic Resonance Imaging. London: SCoR & BAMRR 8. Department of Health (2015). Safety Guidelines for Magnetic Resonance Imaging Equipment in Clinical Use. London: Medicines and Healthcare Products Regulatory Agency.
1. Eccles CL, C ampbell M. (2019, June). Keeping Up with the Hybrid Magnetic Resonance Linear Accelerators: How. Journal of Medical Imaging and Radiation Sciences, 50(2).